B e f o r e :
LADY JUSTICE NICOLA DAVIES
LORD JUSTICE ARNOLD
and
LADY JUSTICE FALK
____________________
Between:
| |
(1) SANDOZ AG AND OTHERS
(2) TEVA PHARMACEUTICAL INDUSTRIES LIMITED AND ANOTHER
(3) CIPLA LIMITED AND ANOTHER
(4) AMAROX LIMITED AND ANOTHER
(5) GENERICS (UK) LIMITED AND ANOTHER
(6) STADA ARZNEIMITTEL AG AND OTHERS
|
Claimants/ Respondents
|
| |
- and -
|
|
| |
(1) BAYER INTELLECTUAL PROPERTY GMBH
(2) BAYER AG
(3) BAYER PLC
|
Defendants/ Appellants
|
____________________
Iain Purvis KC, Miles Copeland and Alice Hart (instructed by A & O Shearman) for the Appellants
Adrian Speck KC, Henry Ward and Adam Gamsa (instructed by Pinsent Masons LLP, Bristows LLP, HGF Law LLP and Taylor Wessing LLP) for the Respondents other than CIPLA Ltd and another
CIPLA Ltd and another were not represented
Hearing date : 16 May 2024
____________________
HTML VERSION OF APPROVED JUDGMENT�
____________________
Crown Copyright ©
This judgment was handed down remotely at 10.30am on 24 May 2024 by circulation to the parties or their representatives by e-mail and by release to the National Archives.
.............................
Lord Justice Arnold:
Introduction
- This is an appeal from an order made by His Honour Judge Hacon sitting as a High Court Judge on 12 April 2024 revoking European Patent (UK) No. 1 845 961 ("the Patent") for the reasons given in his judgment of the same date [2024] EWHC 796 (Pat). The Appellants ("Bayer") are the owner and alleged exclusive licensees of the Patent. The Respondents are various companies which supply generic medicines. The Respondents brought these proceedings claiming an order for revocation of the Patent and Bayer counterclaimed for threatened infringement.
- The Patent claims the use of rivaroxaban for the treatment of a thromboembolic disorder by means of once daily administration. Rivaroxaban is marketed by Bayer under the trade mark Xarelto. It is Bayer's largest-selling drug, and the fourth best-selling drug in the world. Rivaroxaban itself, and its use for the treatment of thromboembolic disorders, were protected first by European Patent No. 1 261 606 and then by a supplementary protection certificate which expired on 1 April 2024. The Respondents all wish to market generic rivaroxaban. If it is valid, the Patent prevents them from supplying generic rivaroxaban for once daily administration, although it does not prevent them from supplying it for twice (or more frequent) daily administration. In addition to the Respondents, a number of other suppliers of generic medicines are also interested in entering this market. As a result of the need for all players to know as soon as possible whether or not the Patent is valid, and for further reasons touched on at the end of this judgment, the hearing of the appeal was expedited. At the conclusion of the hearing the Court announced that the appeal would be dismissed with reasons to follow. This judgment sets out my reasons for reaching that conclusion.
Technical background
- The judge set out the technical background at [8]-[35]. What follows is a slightly abbreviated version of that account.
Haemostasis and thromboembolism
- Haemostasis is a process which gives rise to the formation of blood clots when an individual suffers injury and there is a need to close damage to blood vessels. Haemostasis is a necessary local response to injury, but vascular blood should otherwise flow freely. In healthy humans there is therefore a homeostatic balance, meaning a self-regulating process which adjusts procoagulant and anticoagulant mechanisms to prevailing conditions so as to best ensure the individual's survival.
- Thrombosis is a condition in which a clot, or thrombus, causes obstruction of the blood flow in part of the vascular system away from a site of injury. Thrombosis has long been treated by the administration of anticoagulants.
The coagulation cascade
- Blood has a liquid component, plasma, and three solid components: red blood cells, white blood cells and platelets. The primary purpose of red blood cells is to carry oxygen, but they have a secondary function in that they become passively trapped in thrombi, forming the bulk of a thrombus. The primary purpose of white blood cells is to combat infection. Some classes of one type of white blood cell, leukocytes, express on their surface a protein called "tissue factor" during haemostasis which activates blood coagulation. Platelets are very small cell fragments which, when activated, aggregate and adhere to nearby surfaces, forming part of a thrombus.
- The "coagulation cascade" is the name given to a series of reactions culminating in the formation of an insoluble clot. The enzymes which catalyse the reactions are known as "factors", identified by Roman numerals and given the suffix "a" when the factor is in its active form. The diagram below provides an overview of the coagulation cascade:
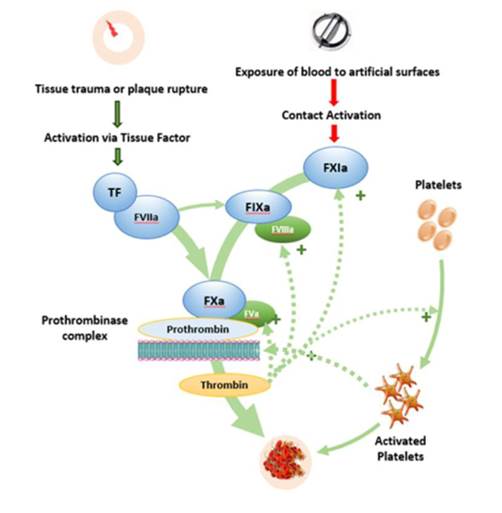
- The upper part of the diagram shows two pathways, each contributing to the activation of Factor X to Factor Xa ("FXa"). The one on the left is known as the extrinsic pathway, the one on the right the intrinsic pathway. FXa in association with Factor Va converts prothrombin (Factor II) to thrombin (Factor IIa). Thrombin feeds back into the cascade to activate other factors and platelets, an effect shown by the dotted lines. Thrombin also converts fibrinogen to fibrin. Fibrin is an insoluble polymer in the form of threads which stabilize the structure of a clot.
Thromboembolic disorders
- The primary causes of thrombosis are the improper functioning of the coagulation cascade and/or excessive platelet activation, commonly because the anticoagulation system is overwhelmed by thrombotic stimuli. A thrombus may break loose and be carried elsewhere in the circulatory system. In that form it is known as an "embolus", and the condition as "embolism". "Thromboembolism" describes the combined conditions of thrombosis and embolism.
- Patients undergoing major surgery are at particularly high risk of venous thromboembolism ("VTE"). One form is deep vein thrombosis ("DVT"), the most serious complication of which is pulmonary embolism ("PE") in the lung. PE remains a significant cause of death in both surgical and non-surgical patients.
- The human body has its own mechanisms to modulate clot formation. There are three, each inactivating factors in the coagulation cascade and in one case also inactivating thrombin. Where urgent anticoagulation in a patient is needed, drugs are used to prevent the formation of thrombi and/or to degrade them.
The therapeutic window
- An important feature of anticoagulant drugs is that, if they are not sufficiently effective, clots will remain and new clots may form. If they are too effective, clots required at the site of injury will not form, particularly after surgery, and the patient will suffer excessive bleeding. Both possibilities are dangerous for the patient and either may be fatal. There is thus a "therapeutic window" in which the drug is sufficiently available and effective to have the desired anticoagulant effect, but not so available and effective such that the patient suffers from unwanted bleeding. The wider the therapeutic window afforded by a drug, the more attractive it is for clinical use. But it is never possible to know in advance where the therapeutic window lies and how wide the window will turn out to be.
Prior art anticoagulant drugs
- The principal anticoagulant drugs in clinical use at the priority date of the Patent, 31 January 2005, were warfarin, heparin (either unfractionated heparin or a low molecular weight heparin ("LMWH") such as enoxaparin) and fondaparinux (an indirect FXa inhibitor). Three other anticoagulants had been licensed for treatment by then, namely hirudin, bivalirudin and argatroban. It was generally known that several new anticoagulants, including two direct FXa inhibitors, were undergoing clinical trials.
Clinical trials
- Drugs undergoing development are subjected to pre-clinical tests which, if successful, will lead to clinical trials. All are mandatory and governed by rules issued by regulatory bodies. Pre-clinical trials include tests as to safety, toxicity and what are sometimes called "proof-of-concept" studies which give an early indication of whether the drug will have the intended effect. Tests will be in vitro or ex vivo and may also involve experiments on animals.
- Clinical trials are carried out in three phases, I to III. Phase I clinical trials are conducted on a small number of healthy volunteers. At the priority date they were almost invariably young males. The primary goal is to obtain data on safety, toxicity and what are called pharmacokinetics (PK) and pharmacodynamics (PD) data. Broadly, PK data measure the effect of the body's system on the drug over time, PD data the effect over time of the drug on the body's system.
- The key PK measurement is the half-life of the drug. Following administration, the drug may be metabolised to an inactive form and will be excreted. Its concentration in blood plasma therefore declines. The rate of decline varies between drugs. As the term implies, the half-life of a drug is the time taken for its concentration in the plasma to decline by half. The PK profile is a graphical representation of the plasma concentration against time from initial administration until it reaches zero. The cumulative exposure of the individual to the drug is shown by the area under the curve or AUC.
- PD data measure the effect over time that the drug has on the patient using "bio-markers", which are measurable indicia associated with the intended effect of the drug.
- There may or may not be a correlation between the half-life of a drug and any one or more PD measurements. Thus, the level recorded from the bio-marker assay may not decline by half at the same time that the drug concentration has halved. Thus PD data may follow a curve different to the PK curve.
- The first Phase I study is usually carried out with the administration of successively ascending single doses. Single ascending dose studies were referred to in the evidence as "SAD studies". Typically these are followed by administering multiple ascending doses, "MAD studies".
- If the Phase I trial is successful, the pharmaceutical research team will move on to Phase II. The cohort of individuals recruited is larger, and unlike those in Phase I they will all have the condition to be treated by the drug being tested. In the case of an anticoagulant, they will typically be patients who have had surgery to replace a knee or hip and who are vulnerable to VTE. The dosage and the frequency of administration will be informed by the results of the Phase I trial.
- If the Phase II trial reveals one or more regimens of dosage and frequency of administration which appear to give satisfactory results, these will be used for a larger Phase III trial. The aim of a Phase III trial is to generate the data required to obtain regulatory approval.
Coagulation assays used for PD studies
- Several assays have been developed to measure the effect of anticoagulants. These are used in pre-clinical studies and for obtaining PD data in Phase I clinical trials. They include:
(1) Prothrombin time or "PT". This measures the time taken to generate fibrin via the extrinsic pathway following activation of Factor VII by tissue factor. It is the test used to monitor the dosage of warfarin. PT is reported as an international normalised ratio or INR.
(2) Activated partial thromboplastin time or "APTT". This measures the time taken to generate fibrin by the intrinsic pathway. Activators of factors in that pathway are used to cause the creation of a clot, subject to addition of the anticoagulant under test which will prolong that time. The time taken is the APTT. APTT was generally used to monitor the activity of heparin.
(3) "HepTest". An excess of FXa is added to the test plasma containing the anticoagulant and to control plasma. After incubation the mixtures are recalcified and the clotting time recorded. It is used to measure levels of unfractionated heparin and LMWHs, and could be adapted to measure direct FXa inhibitors. At the priority date it was not routinely used for patient monitoring, but could be used for research.
(4) FXa assay. A plasma sample is drawn from a subject who has taken an anticoagulant which operates as a FXa inhibitor. The residual FXa left uninhibited is measured using a chromogenic substrate specific for FXa. This was only available in specialised laboratories used for research (such as those run by Bayer), as opposed to labs used for clinical patient monitoring.
- Three other assays were endogenous thrombin potential (ETP), prothrombinase-induced clotting time (PICT) and platelet-induced thrombin generation time (PITT). The judge did not go into detail about these.
- All the foregoing assays measure changes in a biomarker associated with anticoagulation and the effect over time of the drug being tested on that biomarker. The tests are typically carried out ex vivo, which means that successive samples of blood are taken from an individual to whom the drug has been administered and changes in the biomarker are monitored in samples taken over an appropriate period.
- At the priority date none of these had been established as guaranteed predictors of efficacy or safety for direct FXa inhibitors. Nonetheless they were considered useful enough indicators to use in Phase I trials of a potential antithrombotic drug. For a drug known to act by inhibiting FXa, assays that measure FXa level were the most useful.
- Measuring anticoagulation effect in this way is not a direct means of measuring antithrombotic effect, either in the sense of prophylaxis (preventing the formation of thrombi) or treatment (removing thrombi). That can only be done by testing the drug in a patient suffering from or vulnerable to thrombosis, which happens in a Phase II or Phase III trial. Typically this is done using a venogram scan. The scan involves the injection of a contrast dye into the veins under investigation and then examination of the veins by X-ray.
The Patent
- The title of the Patent is "Treatment of thromboembolic disorders with rivaroxaban". The specification refers to the development of drugs which inhibit FXa for the treatment and prophylaxis of thromboembolic disorders. It continues:
"[0009] In general, oral application is the preferable route of administration of a drug, and a less frequent dose regimen is desirable. In particular, once daily oral application is preferred due to favourable convenience for the patient and for compliance reasons. However, this goal is sometimes difficult to achieve depending on the specific behaviour and properties of the drug substance, especially its plasma concentration half life.
[0012] Surprisingly, it has now been found in patients at frequent medication that once daily oral administration of a direct FXa inhibitor with a plasma concentration half life time of 10 hours or less demonstrated efficacy when compared to standard therapy and at the same time was as effective as after twice daily (bid) administration."
- The specification contains a single example, which is a clinical study of rivaroxaban. The specification explains that the purpose of the study was to assess the safety, tolerability, and efficacy of rivaroxaban at different oral doses, administered once or twice daily, compared with 40 mg of subcutaneously administered enoxaparin in the prevention of venous thromboembolism. 642 patients were enrolled, men over 18 years of age and postmenopausal women, all undergoing elective primary hip replacement. It is common ground that this would be recognised as a Phase II clinical trial.
- The specification states that patients either received 40 mg of the comparator, enoxaparin, once daily, or received rivaroxaban according to one of the following regimens: 2.5 mg twice daily, 5 mg twice daily, 10 mg twice daily, 20 mg twice daily, 30 mg twice daily or 30 mg once daily. The duration of the trial was 7-9 days.
- Two tables are presented. The first table sets out efficacy results in terms of the percentage reduction in VTE incidence rates (where (I) means rivaroxaban, bid means twice a day, od means once a day and N provides the number of patients for each regimen):
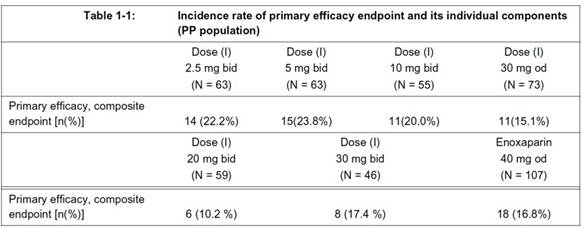
- Beneath the first table in [0044] there is a summary:
"Summary: The above data clearly demonstrate the efficacy of od administration of (I), namely fewer occurrence of composite endpoint events, i.e. fewer cases of DVT, PE or death compared to untreated conditions, and in the range of standard therapy. Furthermore, the od administration is surprisingly perfect in line with bid administration."
- The second table provides safety results in terms of percentage incidence rates of post-operative bleeding:
- Beneath the second table in [0046] there is another summary:
"Summary: The above data clearly demonstrate the safety of od administration of (I). The occurrence of any major bleeding events is low, approximately in the range of standard therapy and again perfectly in line with results from bid administration."
- The only claim which is necessary to consider is claim 1. This is as follows:
"The use of a rapid-release tablet of [rivaroxaban] for the manufacture of a medicament for the treatment of a thromboembolic disorder administered no more than once daily for at least five consecutive days, wherein said compound has a plasma concentration half life of 10 hours or less when orally administered to a human patient."
- It is important to note two points about this claim. First, the claim is not limited to any particular size of dose administered once daily. Secondly, the parties are agreed in these proceedings that the final integer of the claim concerning the half-life is non-limiting and may therefore be ignored.
The skilled team
- It is common ground that the Patent is directed to a team of persons skilled in the art consisting of a pharmacologist and a clinician interested in the treatment of thromboembolic disorders.
The witnesses
- Each side called two expert witnesses, a clinician and a pharmacologist. The Respondents' experts were Professor Jack Hirsh (clinician) and Professor Martin Wilkins (pharmacologist). Bayer's experts were Professor Mark Crowther (clinician) and Professor Bernd Meibohm (pharmacologist). The judge found that (as is common in patent cases) all of the experts were over-qualified, but nevertheless they had each done their best to adopt the mindset of the relevant skilled person at the priority date. The judge also found that all of the experts had done their best to assist the court. The judge rejected two criticisms advanced by Bayer of the way in which the Respondents' experts had been instructed; and, although he considered there was more substance in a third criticism, he found that it had not had any significant effect on the evidence given.
- Bayer called one witness of fact, Dr Frank Misselwitz, formerly Vice-President and Head of the Therapeutic Area of Cardiovascular and Coagulation at Bayer. Dr Misselwitz was one of the authors of, or a contributor to, each of the items of prior art referred to below. He is also one of the inventors named in the Patent. He only gave evidence concerning an issue as to the identification of BAY 59-7939 (as to which, see below).
Common general knowledge
- It is common ground that everything I have set out under the heading "Technical background" was part of the common general knowledge of the skilled team. The judge made findings, none of which are challenged by either side, as to disputed aspects of common general knowledge at [159]-[177]. His findings may be summarised as follows.
The utility of PK and PD data for making predictions
- PK and PD data are informative about likely clinical efficacy, but are not necessarily predictive. Although predictive results can only be produced by Phase II and III trials, the go-ahead for a Phase II trial can be justified by appropriately informative data from one or more Phase I trials.
The significance of the half-life
- PK data showing the half-life of a drug is a starting point for selecting a dosing regimen that will be safe and will afford an effective antithrombotic effect. It is information that will be taken into account along with PD data. It does not necessarily follow that an appropriate regimen will require dosing at a frequency of once every half-life. There are too many uncertainties regarding the effect of a new drug over time for that to be a universal rule of thumb. Moreover, there are guides to the appropriate regimen other than half-life. Nevertheless, half-life is an important contributory guide when beginning the search for a regimen which is both safe and effective.
Selection of regimens for a Phase II trial
- The principal purpose of a Phase II trial, assuming that it appears to show sufficient efficacy and safety, is to establish the optimum dose regimen to take forward into a Phase III study. This will involve trying a range of dose regimens. No dose would be used in the expectation that it would put patients at risk. Subject to that, it may be expected that some doses will turn out to be less effective than others.
Making predictions about the therapeutic window
- The skilled team would not have made predictions about the therapeutic window of rivaroxaban based on heparin data because such data was not common general knowledge. The same was true of information concerning other FXa inhibitors.
Once daily administration
- The skilled team would have been aware of the clinical advantages of a once daily tablet in terms of patient adherence and convenience over, say, a twice daily tablet. They would also have been aware of the potential financial advantage that would flow from marketing the first once daily tablet for thromboembolic disorders. However, both considerations would have been secondary to safety concerns when designing a Phase II clinical trial.
The ribbon
- The skilled team conducting a Phase II study with no knowledge of the size of the therapeutic window would aim for a relatively small peak-to-trough difference in the concentration of the drug in the plasma. This would increase the chance of the "ribbon" falling safely within the therapeutic window. The ribbon was the name given in argument to the wavy line graphically representing drug concentration in the plasma over time after steady state has been reached, oscillating between maxima and minima.
- Prof Meibohm illustrated this point with the following graph showing a hypothetical therapeutic window of 10-20 mg/L (shown by the dotted horizontal lines) and two regimens A (three times daily at a lower dose) and B (once daily at a higher dose) for administration of the same overall dose of a drug:
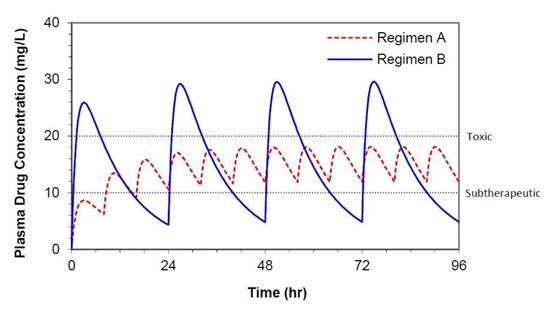
- Two points should be noted about this graph. The first is that steady state is only reached after more than 24 hours. The second is that the graph appears to suggest that regimen A has been selected in order to fall within a known therapeutic window, but in reality the position and size of the therapeutic window would not be known.
- Prof Meibohm explained that doubling the dose and halving the frequency of administration would double the peak-to-trough distance, i.e. double the width of the ribbon. Conversely, halving the dose and doubling the frequency of dose would halve the width of the ribbon. He accepted, however, that the peak-to-trough variation in drug concentration is determined by the dose, and that, if one increases the frequency of dosing with the same dose, the steady state will settle at a higher level.
- The judge nevertheless accepted at [176] Prof Meibohm's evidence that the skilled team contemplating a Phase II trial with rivaroxaban, based on the Phase I data in the prior art, would know that administering a relatively low dose at relatively high frequency would result in a narrower ribbon and a better chance of staying safely inside the therapeutic window wherever it turned out to be.
The prior art
- The prior art relied upon by the Respondents is a poster entitled "Effects of BAY 59-7939, an Oral, Direct FXa Inhibitor, on Thrombin Generation in Healthy Volunteers" by Sebastian Harder and nine co-authors ("Harder"), which was presented at the 45th Annual Meeting of the American Society of Hematology in San Diego, USA, on 6-9 December 2003. Harder identifies the first three named authors as being affiliated with the Institute of Clinical Pharmacology, University Hospital, Frankfurt am Main, Germany, the next six authors as being affiliated with Bayer and the last author, Hans-Klaus Breddin, as being affiliated with the Institute of Thrombosis and Vascular Diseases, Frankfurt. The judge found that, at the priority date, the skilled team would have discovered the identity and chemical structure of BAY 59-7939, which is now known as rivaroxaban. There is no challenge by Bayer to that finding.
- It was common ground that Harder would be read together with the corresponding abstract: "Effects of BAY 59-7939, an Oral, Direct FXa Inhibitor, on Thrombin Generation in Healthy Volunteers", Blood, 2003, 102(11), 811a, Abstract 3003 ("Blood 3003").
- The judge found that Harder would also be read together with two posters by Dagmar Kubitza and four co-authors ("the Kubitza posters") which were presented at the same meeting and which are cited in Harder. There is no challenge by either side to that finding. All bar one of the authors of the Kubitza posters were also authors of Harder. In addition, Dr Misselwitz, who contributed an introduction to each of the Kubitza posters, was also an author of Harder. To complete the picture, Dr Kubitza is also one of the named inventors of the Patent.
Harder
- Harder begins, under the heading "Introduction":
"BAY 59-7939 is a selective, highly potent, direct Factor Xa (FXa) inhibitor that is being developed for the prevention and treatment of thromboembolic disease. It has been shown to be well tolerated at single and multiple doses up to 30 mg, and is rapidly absorbed after oral administration, with a terminal half-life of 9-12 hours."
- It continues, under the heading "Objective":
"The aim of this study was to evaluate the effect of orally administered BAY 59-7939 on thrombin generation in healthy male volunteers."
- Under the heading "Subjects and methods", the reader is told that the study was conducted on 12 healthy male subjects aged between 27 and 37. BAY 59-7939 was administered to eight of them while four had a placebo. The eight received a single 5 mg oral dose on day 1 and a single 30 mg oral dose on day 14 (i.e. sufficiently later for the first dose to have been expelled from the body), or vice versa. Assessments of thrombin generation and platelet-inducing clotting were performed over 24 hours. Details of how the assessments were done are then given. There were three: a PITT assay, an ETP assay and a PICT assay.
- Under the heading "Results", Harder states:
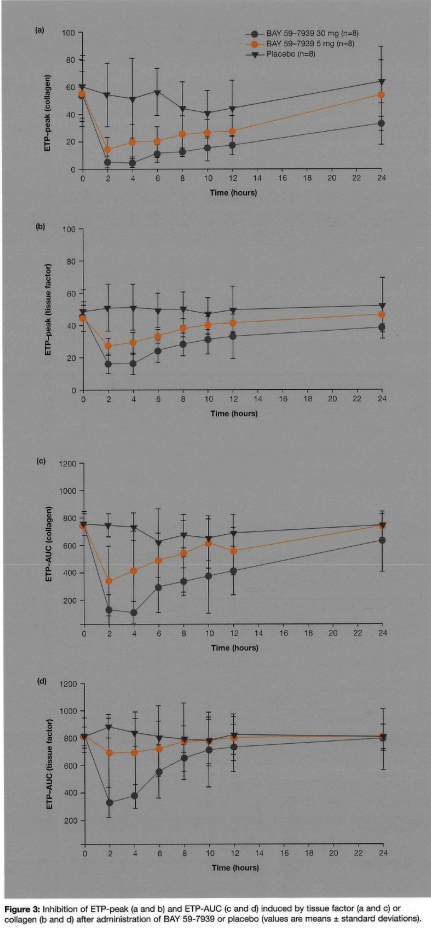
"ETP (peak or AUC) was reduced significantly (compared with placebo profiles) by both the 5 mg and 30 mg doses of BAY 59-7939, with maximum effect at 2-4 hours. Inhibition of ETP-peak and ETP-AUC (induced by tissue factor or collagen) by 30 mg BAY 59-7939 was sustained over 12 hours (Figure 3)."
- Figure 3 is reproduced below. It illustrates the effect of 5 mg and 30 mg doses of BAY 59-7939 on thrombin activity measured by ETP compared with a placebo. Graphs (a) and (b) show ETP peak values, graphs (c) and (d) show AUC. Graphs (a) and (c) show the values where ETP was induced by collagen, while in graphs (b) and (d) it was induced by tissue factor.
- Harder goes on:
"PITT (Tc) was prolonged significantly (compared with placebo profiles) by the 30 mg dose of BAY 59-7939. Maximal prolongation of Tc was approximately 2-fold by 5 mg BAY 59-7939 and approximately 4-fold by the 30 mg dose (compared with placebo group), and was observed 2-4 hours after dose administration. The increase in PITT was sustained by 30 mg BAY 59-7939 over 12 hours (Figure 4a)."
- It then says:
"PICT was prolonged significantly (compared with placebo profiles) by both the 5 mg and 30 mg doses of BAY 59-7939. Maximal prolongation was approximately 2-fold by 5 mg BAY 59-7939 and 3-fold by the 30 mg dose, and was observed 2 hours after administration. PICT was prolonged over 12 hours after treatment with 5 mg and 30 mg BAY 59-7939 (Figure 4b)."
- Figure 4, like Figure 3, shows plots for the PITT and PICT results at 24 hours, and, like Figure 3, suggests some residual activity after 24 hours.
- Harder continues:
"In agreement with other phase I data [the Kubitza posters], FXa was inhibited dose dependently after administration of BAY 59-7939. Maximum inhibition was observed 2 hours after treatment (28% and 56% inhibition after treatment with 5 mg and 30 mg BAY 59-7939, respectively). FXa inhibition correlated closely with ETP, as demonstrated by the values of the ETP-peak."
- Under the heading "Conclusions", Harder states (omitting a footnote):
"• Orally administered BAY 59-7939 dose-dependently inhibited both intrinsic (collagen) and extrinsic (tissue factor) pathways of thrombin generation.
• The effect of BAY 59-7939 on thrombin generation was demonstrated in platelet-free assays and in PRP-based assays. In contrast, indirect (i.e. antithrombin III-dependent) FXa inhibitors obviously only inhibit FXa that is not protected by the platelet-prothrombinase complex.
• BAY 59-7939 not only inhibited the lag time of thrombin generation (PITT-T�c), but also had a profound effect on both the maximum extent of thrombin generation (ETP-peak) and the total amount of generated thrombin (ETP-AUC). This observation suggests an additional feature of BAY 59-7939, because weaker FXa inhibitors may only prolong lag-time without affecting the total amount of thrombin generation.
• Some parameters (e.g. ETP-peak) indicate a long-lasting pharmacodynamic effect of BAY 59-7939, which suggests suitability for a once-daily dosing regimen.
• The effects of oral BAY 59-7939 on intrinsic and extrinsic thrombin generation and PICT, which are mediated by direct inhibition of FXa, indicate that BAY 59-7939 is a promising anticoagulant that merits further clinical investigation."
Blood 3003
- Blood 3003 is a summary of Harder. The only point that it is necessary to note is that it states:
"A single 30 mg dose exerted a sustained effect in some assays of thrombin generation for up to 24 hours."
The Kubitza posters
- There are two Kubitza posters, both in a similar format to that of the Harder poster but with more detail. The first is entitled "Single Dose Escalation Study Investigating the Pharmacodynamics, Safety and Pharmacokinetics of BAY 59-7939 an Oral, Direct FXa inhibitor in Healthy Male Subjects". The title of the second is the same, save that it is a "Multiple Dose Escalation Study". As their titles imply, they differ in that the first involved SAD administration of the drug or a placebo over the period of the study while the second involved MAD administration.
- The SAD study was carried out on 103 healthy men under fasting conditions. Some received BAY 59-7939 in 9 steps, being successive doses of 1.25, 5, 10, 15, 20, 30, 40, 60 and 80 mg tablets. BAY 59-7939 was administered to others in two oral solutions of 5 and then 10 mg. Yet others received placebos.
- As is explained under the heading "Subjects and methods", pharmacodynamic and pharmacokinetic tests of the volunteers' blood were carried out as follows:
"• Pharmacodynamic effects were evaluated using FXa activity, prothrombin time (PT), activated partial thromboplastin time (aPTT) and HepTest; selectivity was assessed by measuring Factor IIa (FIIa) and antithrombin III activity.
• The pharmacokinetic parameters measured included area under the plasma concentration-time curve from zero to infinity (AUC) maximum drug concentration in plasma (Cmax), and half-life associated with terminal slope (t1/2)."
- The results from the pharmacodynamics are given, and in the case of FXa activity this includes duration:
"All pharmacodynamic parameters had similar dose-dependent time-response curves, although the magnitude of the curves varied depending on the parameter. Overall, pharmacodynamic parameters were slightly more affected after administration of oral solution than after tablet administration.
FXa activity and specificity
Median FXa inhibition ranged from 20% for 5 mg tablets to 61% for 80 mg tablets (Figure 1). The maximum inhibitory effect on FXa activity was observed 1-4 hours after tablet administration, and returned to the normal range (0.7-1.2 U/mL) within 24 hours for doses up to 40 mg. [Inhibition of] FXa activity remained elevated beyond 24 hours for the 60 mg and 80mg doses. BAY 59-7939 was specific for FXa and did not affect FIIa (Figure 2) or antithrombin III (Figure 3)."
- Figure 1 is reproduced below:
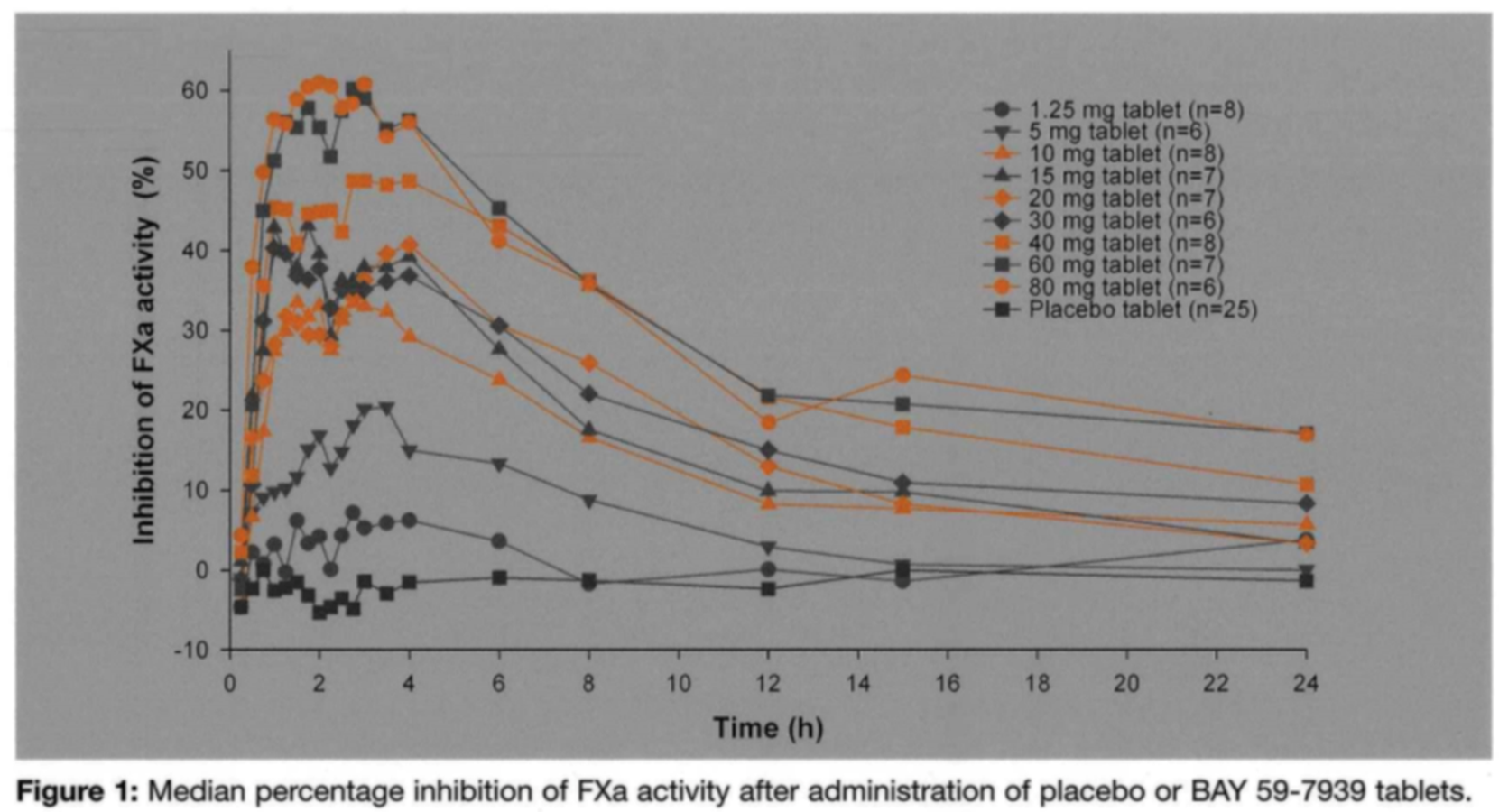
- The judge found that the skilled team would have noticed from Figure 1 that inhibition of FXa is shown to remain elevated above the baseline at 24 hours for the 30 and 40 mg doses as well as the 60 and 80 mg doses. The same appears to be true of the PT assay.
- The pharmacokinetic results include an estimate of the half-life of BAY 59-7939 in the volunteers' plasma when administered as an oral solution (no half-life estimation for tablets is given):
"Plasma concentration-time profiles showed rapid absorption after administration of the solution. Maximal plasma concentrations were achieved after 30 minutes and t1/2 was estimated to be 3-4 hours."
- FXa inhibition is plotted against plasma concentration, showing a close correlation at higher plasma concentrations. At low plasma concentrations, small increases in plasma concentration are shown to cause a relatively large increase in FXa inhibition. PT results are also plotted against plasma concentrations, showing a consistent close correlation.
- The poster states in its conclusions that a "close correlation was observed" between PD effects and plasma concentrations. The poster also concludes that the results reported "indicate that further investigation of BAY 59-7939 is warranted".
- The MAD study was with 64 subjects, of whom 61 also took part in pharmacokinetic analyses. The volunteers were each randomly assigned to active treatment or administration of a placebo. Treatment was in six steps, the first on day 1 and then on days 4-8. For those receiving BAY 59-7939, the successive daily dosing regimens were: 5 mg once, 5 mg twice, 5 mg three times and then 10 mg, 20 mg and 30 mg in each case twice daily. Pharmacodynamic (FXa activity, PT, APTT and HepTest) and pharmacokinetic tests were conducted along similar lines to those in the SAD study.
- Inhibition of FXa was slightly above baseline after 24 hours with the twice-daily administration of the highest dose used (30 mg). FXa inhibition also remained slightly above the baseline 24 hours after the final dose. This correlated with plasma concentrations of the drug, which also remained above the baseline 24 hours after the final dose. Similar sustained effects could be observed in relation to PT. The judge accepted Prof Hirsh's evidence that the skilled clinician would consider that these data were consistent with the prolonged pharmacodynamic effects seen in the 30 mg dose in the SAD study and with the sustained effects at 24 hours in some of the thrombin generation assays seen at this dose in Harder.
- The poster reported:
"• Cmax was reached 2.5-4 hours after administration, and the [half-life] of the 5 mg dose was 5.4 hours.
• For the 10 mg and 30 mg doses, the mean [half-life] was 5.8 hours, and for the 20 mg dose it was 3.7 hours."
- As with the SAD study, FXa inhibition and PT results were plotted against plasma concentration. The results were similar.
- The poster's conclusions are as follows:
"• BAY 59-7939 was safe and well tolerated after multiple-dose administration at all the doses tested without signs or symptoms of bleeding. BAY 59-7939 inhibited FXa activity and dose-dependently affected the pharmacodynamic parameters PT, aPTT and HepTest.
• Predictable dose-dependent pharmacodynamics and pharmacokinetics were demonstrated, and indicated that BAY 59-7939 is suitable for twice-daily administration up to 30 mg.
• Close correlation existed between the prolongation of the PT and plasma concentrations
• The good safety profile, selective inhibition of FXa and promising pharmacokinetic and pharmacodynamic profiles indicate that further investigation of BAY 59-7939 is warranted."
The law on obviousness
- There was no dispute either before the judge or this Court as to the applicable legal principles. A claimed invention lacks an inventive step, and therefore the claim is invalid, if it would be obvious to the skilled person or team having regard to the prior art read in the light of their common general knowledge. As Kitchin J said in Generics (UK) Ltd v H. Lundbeck A/S [2007] EWHC 1040 (Pat) at [72], approved by the House of Lords in Conor Medsystems Inc v Angiotech Pharmaceuticals Inc [2008] UKHL 49, [2008] RPC 28 at [42] (Lord Hoffmann) and by the Supreme Court in Actavis Group PTC EHF v ICOS Corporation [2019] UKSC 15, [2019] Bus LR 1318 at [63] (Lord Hodge):
"The question of obviousness must be considered on the facts of each case. The court must consider the weight to be attached to any particular factor in the light of all the relevant circumstances. These may include such matters as the motive to find a solution to the problem the patent addresses, the number and extent of the possible avenues of research, the effort involved in pursuing them and the expectation of success."
- The same legal standard is applicable when determining the obviousness of a dosing claim as with any other claim: see Actavis v ICOS at [42]. As Lord Hodge explained in Actavis v ICOS at [65]:
"
it is relevant to consider whether at the priority date something was 'obvious to try', in other words whether it was obvious to undertake a specific piece of research which had a reasonable or fair prospect of success: Conor v Angiotech, para 42 per Lord Hoffmann; MedImmune Ltd v Novartis Pharmaceuticals UK Ltd [2012] EWCA Civ 1234; [2013] RPC 27, paras 90 and 91 per Kitchin LJ. In many cases the consideration that there is a likelihood of success which is sufficient to warrant an actual trial is an important pointer to obviousness. But as Kitchin LJ said in Novartis AG v Generics (UK) Ltd [2012] EWCA Civ 1623, para 55, there is no requirement that it is manifest that a test ought to work; that would impose a straightjacket which would preclude a finding of obviousness in a case where the results of an entirely routine test are unpredictable. As Birss J observed in this case (para 276), some experiments which are undertaken without any particular expectation as to result are obvious. The relevance of the 'obvious to try' consideration and its weight when balanced against other relevant considerations depend on the particular facts of the case."
The judge's assessment
- The judge began at [114]-[118] by summarising the issue. He noted that it was common ground that the skilled team would have recognised that Harder and the Kubitza posters were reporting the results of Phase I trials, and that the skilled team having read those documents would have carried out a Phase II trial of rivaroxaban. The judge found that rapid-release rivaroxaban would be used for such a trial, and there is no challenge by Bayer to that finding. Otherwise, it was common ground that, if the skilled team decided to include once daily administration of rivaroxaban in the trial, it would have been used as specified in claim 1 of the Patent. There was no dispute that the skilled team would have considered whether to include once daily administration as a regimen in the Phase II trial. The only issue was whether the skilled team would have had a reasonable expectation of success with respect to once daily administration.
- The judge next considered at [119]-[132] what was meant by "success" in this context. Having noted that the skilled team would not know where the therapeutic window lay, how wide it was or what dosing regimens would result in the effect of the drug falling within the window, he went on:
"121. The difficulty is quite marked in relation to an anticoagulant such as rivaroxaban. As I have discussed, administering the new drug in a dosage that was too low posed a real risk of harm to patients in the study. Due to invasive surgery or for other reasons they would be vulnerable to clot formation. If such formation were not inhibited, or not sufficiently inhibited, a fatal thromboembolism in the brain or a lung or elsewhere could be the result. Equally, a high dose causing excessive anticoagulant activity could lead to bleeding, not just at the site of a wound but elsewhere, such as the brain, again leading to harm and even, potentially, the patient's death.
122. The hypothetical team planning a phase II trial on the back of Bayer's phase I data would therefore have approached the trial with caution. If the team were to have considered trying a once daily dosing regimen, a reasonable expectation of success would have amounted to a reasonable expectation that such a regimen would not put the welfare of the patients in the phase II trial at unacceptable risk."
- The judge then explained that it had occurred to him during his reading for the trial that an unusual feature of the present case was the basis on which Bayer appeared to be claiming an inventive step:
"124. In the present case there would have been no
perceived technical barrier to the claimed invention on the part of the skilled team. The team would have known that it could conduct a phase II trial using a wide range of once-daily doses from one small enough to be sure that there is no excessive bleeding up to a dose large enough to be sure of an antithrombotic effect over 24 hours. Such a range would have been likely to find the therapeutic window somewhere in the lucky patients administered with one of the doses fitting the window.
125. Rather, the skilled team here would have been held back (if that was the case) by an ethical barrier. Since the size and location of the therapeutic window was unknown, administration of a wide range of once-daily doses would have posed a real risk of including one or more that missed the window, causing harm to patients."
- Clinical trials can only be carried out if approved by an ethics committee, however. The relevant ethics committee must have approved the carrying out by Bayer of the Phase II trial reported in the Patent. That committee must therefore have been satisfied that patients' lives would not be put at unacceptable risk. The judge went on:
"129. Given that the ethical question will be resolved by an ethics committee rather than the skilled team, the real criterion in the present case is whether the skilled team would have thought that it was worth applying to the committee for permission to conduct a phase II trial which included a once-daily regimen with a reasonable expectation that the committee would give permission, and whether it was likely that permission would be given.
130. The case was not argued in that way. The criterion applied was just whether there would have been a reasonable expectation on the part of the skilled team that a once-daily dose falling would be both safe and effective. Of course, this and the two-part criterion just mentioned could on one view be seen to amount to the same thing."
- The judge then considered at [133]-[158] what he termed "the invention story". The judge explained that he had been referred to decisions of a number of foreign courts in parallel cases. The Board of Appeal of the European Patent Office had maintained the Patent as granted, first instance courts in Australia, Belgium, the Netherlands (twice), Norway and Sweden had held that the claimed invention did not lack an inventive step and the preliminary opinion of the German Federal Patent Court was the same. On the other hand, first instance courts in France and South Africa had reached the opposite conclusion. The judge expressed the view that these decisions were of little assistance to him because they were based on different evidence and arguments.
- The judge nevertheless recorded that the Respondents had submitted that the courts which had found the parallel patents valid had been influenced by Bayer's "invention story". For example, in Belgium Dr Misselwitz provided written evidence to the effect that a first Phase II trial was carried out solely with twice daily and thrice daily dosing, but during the course of this study he had had the idea of trying once daily administration. Initially his idea met with resistance, but eventually he was able to persuade the doubters after an enoxaparin interaction study had been carried out which provided the investigators and the ethics committee with the confidence that, in an emergency caused by an underdosing of rivaroxaban, enoxaparin could be administered in addition to rivaroxaban without complications. Dr Misselwitz was not cross-examined on this evidence. Nor did it appear that Bayer had disclosed the underlying documents.
- Although Dr Misselwitz gave evidence before the judge, he said nothing about this "invention story". The Respondents suggested that this was because Collis J sitting in the Court of the Commissioner of Patents for the Republic of South Africa had been critical of evidence on this point given by Dr Misselwitz at an earlier stage of those proceedings (although Dr Misselwitz was not called as a witness before Collis J). Having set out Collis J's findings, the judge said at [158]:
"I am not in a position to accept Collis J's findings or to reach any view on them. I note however that the invention story or a version of it was advanced before the judge and that she rejected it, reaching the conclusion that for the reasons she gave, Bayer's phase II study was based on their phase I data."
- At [203]-[212] the judge considered four alleged or actual differences relied upon by Bayer between the Phase I data reported in Harder and the Kubitza posters on the one hand and the Phase II use of rivaroxaban covered by the claims of the Patent. The judge held that the only one of these which was material was the fact the Phase I trial involved healthy volunteers, and therefore considerable caution was required when designing a Phase II trial. He reiterated at [213]:
"The only real issue in the case on inventive step was whether it was obvious for the skilled team to conduct a phase II trial which included once daily dosing having read Harder and the Kubitza posters."
- At [214]-[229] the judge summarised the evidence of the experts on once daily administration. In brief, Prof Wilkins and Prof Hirsh each gave evidence to the effect that, based on Harder and the Kubitza posters, the skilled team would include a 30 mg once daily dose in a Phase II trial in addition to smaller twice daily doses such as 5 mg and 15 mg. The skilled team would have a reasonable expectation of success in terms of both efficacy and safety. Both experts had formed that opinion before seeing the Patent. Prof Meibohm said that the pharmacologist would defer to the clinician as to whether to carry out a Phase II trial at all; but if a trial was carried out, they would consider using two twice daily doses, namely 20 mg and 30 mg. Prof Crowther's opinion was that the data in Harder and the Kubitza posters was insufficient for the clinician to consider taking BAY 59-7939 forward to a Phase II trial at all, but if one was carried out the clinician would expect it to be necessary to administer the drug at least twice daily.
- At [230]-[239] the judge summarised the parties' arguments. When setting out the main points made by the Respondents, the judge said at [231]:
"First, the authors of Harder, two clinicians stated by Professor Crowther to be of international renown and scientists from a world-leading pharmaceutical company, told the reader expressly that the data disclosed suggested the suitability of BAY 59-7939 for once-daily dosing."
- The judge set out his analysis and conclusions at [240]-[260]. Although he reverted to the ethical dimension to the case, he noted at [241] that:
"The parties argued the case according to whether the skilled team would have thought that [a once daily] regimen was worth trying in a phase II trial with a reasonable expectation of success, where success would mean that such a regimen would be both sufficiently safe and sufficiently effective in a phase II study."
- The judge went on at [243]:
"
data from a phase I trial can never be predictive of what may happen in a phase II trial. In the case of a study involving a drug for treating thromboembolic disorders a phase I trial of the type disclosed in Harder and the Kubitza posters can only test anticoagulant activity ex vivo. That is not the same thing as, and need not necessarily correlate closely with, antithrombotic activity. The results of the trial do not strictly prove anything with regard to antithrombotic activity. A highly risk averse approach would mean that phase II trials would seldom if ever be conducted. That would not be in the public interest and is clearly not the approach adopted in the real world."
- Having said that the public interest in having new and valuable drugs progress through the pipeline of clinical testing to become available to patients had to be balanced against the risks to individuals in the clinical trials, the judge continued at [245]:
"With that in mind, I turn to the question whether the skilled team
would have considered that there was a reasonable expectation that a once daily regimen, using any chosen dose, would be sufficiently safe by avoiding an unacceptable risk of bleeding and also sufficiently effective by avoiding an unacceptable risk of thromboembolism during the course of a phase II trial."
- The judge began his evaluation of the answer to this question at [247]:
"A problem I have with the evidence of Professors Crowther and Meibohm taken together is that theirs was primarily a counsel of despair. Taken jointly, as it should be, their evidence was that the data from Harder and the Kubitza posters would have led the skilled team to abandon the idea of a phase II trial altogether. Of course, the quality of phase I data must vary from study to study and in theory this data could have been of a quality below the threshold required to go ahead with any sort of phase II study. But even Bayer's counsel in oral submissions was not prepared to go that far. He accepted that the skilled team would not only have contemplated a phase II trial, it would have conducted one. The only issue was whether it would have included a once daily regimen. This does not mean that the evidence of Professors Crowther and Meibohm was of no value it was both valuable and helpful and they had a fallback position on the assumption, of which they disapproved, that the skilled team would have conducted a phase II trial, evidence which I have taken into account. But it seemed to me that there was to some extent a determination to be negative."
- Next, the judge reiterated that the skilled team would have been aware of the clinical advantages and potential financial benefit of a once daily tablet. Those factors would have been secondary to the team's safety concerns, but they meant that, where the prior art raised the possibility of including a once daily regimen in a Phase II trial, that possibility would have been given serious consideration.
- The judge then reasoned as follows:
"249. It follows that the skilled team would have found the statement in Harder that some parameters investigated in the document suggested the 'suitability [of orally administered BAY 59-7939] for a once-daily dosing regimen' both striking and encouraging. The authors of Harder were either, like Dr Harder himself, distinguished clinicians of apparently international renown or, like Dr Misselwitz, senior figures in Bayer, very much a leader in the field. The skilled team would in my view have considered carefully why these authors had been prepared to put their names to that statement. Further, Blood 3003
said that some assays pointed to an anticoagulant effect lasting 24 hours after a single 30 mg dose.
250. The skilled team would have been likely to consider first the reported evidence on the half-life of BAY 59-7939. Harder reported a figure of 9-12 hours, supportive of the idea of once daily dosing. But as Professors Crowther and Meibohm pointed out, there was no PK data to support it and the study involved only 8 participants treated with BAY 59-7939. The numbers of volunteers in both the Kubitza posters were much larger and there was supporting data. The figures of 3.7 and 5.8 hours in the two Kubitza posters would have been seen as more reliable.
251. The authors of Harder must have had the data in the Kubitza posters in mind when the statement regarding suitability for once daily dosing was made. Harder refers to the data of the Kubitza posters as being supporting of at least some of the PD data reported in Harder. And the authors would probably not have pointed out that some data supported once daily dosing if such data were to be dismissed as of no value because of other data in Harder and/or the Kubitza posters.
252. The skilled team would therefore have turned to the PD data. Harder stated that the ETP results showed that the inhibitory effect of BAY 59-7939 was sustained over 12 hours. As Professor Hirsh said, the graphical evidence gave some limited support for a sustained anticoagulant effect over 24 hours, although the authors had not seen fit to state this and the error bars meant that the evidence may not have had statistical significance.
253. The larger and therefore more reliable studies in the two Kubitza posters suggested in their graphs that anticoagulant effect as measure[d] by some parameters was significantly sustained 24 hours after administration in the case of 30, 40 and 60 mg doses. On the other hand these posters also concluded that anticoagulant activity according to a PD assay was closely correlated to plasma concentrations. The apparent contradiction, if it was seen as such by the experts, was not directly confronted. I note that the graphs in the Kubitza posters show that at low plasma concentrations of BAY 59-7939 there is not a close correlation between concentration and FXa inhibition. Even at zero concentration prothrombin time did not fall to zero. It could be that at the low plasma levels expected 24 hours after administration anticoagulant activity would no longer have been expected to correlate with plasma levels of BAY 59-7939, but the detail of the graphs was not addressed. As against that, it was resolved in the evidence of Professors Hirsh and Wilkins, and conceded by Professor Meibohm,
that the SAD Kubitza study shows graphical evidence of anticoagulant activity 24 hours after administration, including 24 hours after administration of a 30 mg dose.
254. Taking all the evidence together, I think that the skilled team would have believed that it was reasonable for the authors of Harder to say that there was data in Harder and the Kubitza posters which suggested that BAY 59-7939 was suitable for orally administered once daily administration. That left the question whether the data indicated that there was a dose which would be both safe and effective.
255. The experts were agreed that the data indicated a wide tolerance of BAY 59-7939 in healthy patients, up to a dose of 80 mg. A once-daily dose of 60 or 80 mg would be the most likely to prove effective in treating and preventing thrombi in phase II patients, though high doses of that order were more likely than lower doses to cause excessive bleeding. The question would have been whether the data provided sufficient support for a lower once daily dose that would have a sufficiently sustained antithrombotic effect over 24 hours.
256. In my judgment, the overall views taken by Professors Hirsh and Wilkins in this regard were the more realistic. The data in Harder and the Kubitza posters gave reasonable grounds for the belief that a once daily dose of 30 mg would be likely to have a sustained effect over 24 hours. The data as a whole offered no reason to believe that such a regimen would cause excessive bleeding. Neither the possibility of excessive bleeding nor insufficient efficacy could be completely ruled out with such a regimen, but as I have discussed, some risk was inevitable.
257. Therefore I think that the combined evidence of Professors Hirsh and Wilkins was correct in taking the position that the skilled team would have believed that conducting a phase II trial which included a 30 mg once daily regimen would not have caused an unacceptable level of risk.
258. It follows that the skilled team would have found it obvious to conduct a phase II trial which included such a regimen."
- Having reached that conclusion, the judge added at [259] that, so far as one could tell from the Patent, Bayer had carried out a single Phase II trial which included a once daily 30 mg regimen. That was presumably based on Bayer's Phase I studies reported in Harder and the Kubitza posters. No reason had been advanced as to why the skilled team would not have done the same thing as Bayer did. At [260] the judge recorded that counsel for Bayer had submitted that Bayer must have had more data than was reported in Harder and the Kubitza posters on which to base their design of the Phase II trial, but noted that there was no disclosure by Bayer or evidence from Dr Misselwitz to support that submission.
The appeal
- Obviousness involves a multi-factorial evaluation and therefore this Court is not justified in intervening in the absence of an error of law or principle on the part of the judge: see Actavis v ICOS at [78]-[81]. Bayer face three further difficulties on this appeal. First, the judge's judgment contains a very careful, detailed and nuanced appraisal of the evidence and arguments. Secondly, the judge's decision was in the end squarely based on preferring the evidence of the Respondents' experts to that of Bayer's experts. Thirdly, the judge's preference for the evidence of the Respondents' experts is not surprising. It is a striking feature of this case that, in closing submissions before the judge, counsel for Bayer did not feel able to support the primary position taken by Bayer's experts, namely that the skilled team would not, after having read Harder together with the Kubitza posters, progress rivaroxaban to a Phase II trial at all. That was an extraordinary conclusion to reach when all three posters were positive in tenor.
- Bayer were given permission to appeal on two grounds, grounds 1 and 5. Ground 1 embraces three sub-grounds. Permission to appeal on grounds 2, 3 and 4 was refused. Subsequently Bayer applied for permission to amend their grounds of appeal to raise a new ground. The Respondents resisted the application. We heard full argument on the proposed new ground. Counsel for Bayer also advanced a further ground in oral argument without even applying to amend Bayer's grounds of appeal. I will refer to this as the unpleaded ground. Again, we heard full argument on it despite the absence of any amendment application.
An irrelevant contention
- Before turning to the grounds of appeal, the application to amend and the unpleaded ground, it is convenient to get out of the way a contention advanced by Bayer which is irrelevant to the issue of obviousness. Bayer contend that it was the unchallenged evidence of their expert witnesses that it was surprising, given the data in Harder and the Kubitza posters, that rivaroxaban can be administered once daily as efficaciously and safely as twice daily. Even if this is correct, it is irrelevant. This is because the issue is whether the skilled team would have had a reasonable expectation that once daily administration would be sufficiently efficacious and safe to include it in a Phase II trial in addition to twice daily administration. In considering that question it is important to bear in mind that, as the judge found, it is conventional to include a range of dosing regimens in Phase II trials in order to identify the best regimen to take forward into a Phase III trial.
The application to amend the grounds of appeal
- Formally, Bayer's application to amend their grounds of appeal is to add a new sub-ground to ground 1, but in substance the new paragraph raises an entirely distinct ground of appeal. This is that the judge was wrong to find in [249] that "[t]he authors of Harder were either, like Dr Harder himself, distinguished clinicians of apparently international renown or, like Dr Misselwitz, senior figures in Bayer, very much a leader in the field".
- This is a challenge to a primary finding of fact. It follows that it can only succeed if that finding was rationally insupportable: Volpi v Volpi [2022] EWCA Civ 464, [2022] 4 WLR 48 at [2](v) (Lewison LJ). Furthermore, even if the finding of fact is wrong, Bayer must show that the error materially affected the judge's assessment of obviousness.
- It is convenient to take the elements of the finding in reverse order. First, Bayer say that the judge was wrong to find that Bayer was "very much a leader in the field" because the evidence is that Bayer was new to the field of thromboembolism in 2003. I don't think that the judge meant that Bayer was a leader in the field of thromboembolism. In my view he was accepting the Respondents' point which he recorded at [231] that Bayer were a world-leading pharmaceutical company. Bayer do not dispute that characterisation.
- Next, Bayer say that the judge was wrong implicitly to find that the skilled team would be aware that Dr Misselwitz and his colleagues were senior figures at Bayer. It is not in dispute that Dr Misselwitz was in fact a senior figure: he joined Bayer in April 2002 as Global Clinical Strategist and Global Clinical Leader and became Vice-President and Head of the Therapeutic Area some time in 2005. Bayer are correct that there is no evidence that the skilled team would have known what position Dr Misselwitz held. In my view, however, the skilled team would have inferred from Harder and the Kubitza posters that he was a person of some seniority for two reasons. First, his affiliation is stated to be "Global Medical Development, Bayer HealthCare". Secondly, he is credited as having written the introduction to the Kubitza posters.
- Lastly, Bayer say that the judge was wrong to find that Dr Harder was a distinguished clinician of apparently international renown. Dr Misselwitz gave evidence that at the priority date Dr Harder was a principal investigator at the Institute of Clinical Pharmacology in Frankfurt. Bayer are correct that there is no evidence that Dr Harder had an international reputation, although Prof Meibohm did appear to accept that Dr Harder had "status in the field". Bayer do not dispute, however, that Professor Breddin was an internationally known academic and clinician in the field of thromboembolism who was Director of the Division of Angiology at Frankfurt University and a founding Director of the International Institute of Thrombosis and Vascular Diseases. Thus at least one of the authors of Harder was indeed a distinguished clinician of international renown.
- In summary, therefore, the judge's finding was not merely rationally supportable, but in substance correct even though it could have been more accurately expressed. In any event, the only relevance of the finding to the judge's assessment was that the judge went on to find that the skilled team would have considered carefully why the authors of Harder had been prepared to put their names to the statement that rivaroxaban was suitable for once daily dosing. The judge did not find that, due to the status of the authors, the skilled team would simply take that statement at face value. On the contrary, he found that they would have considered whether there was data in Harder and the Kubitza posters to support it. Since that finding accords with both sides' case, the finding of which Bayer complain did not materially affect his assessment. This may explain why this ground did not feature in Bayer's original grounds of appeal.
- I would therefore refuse Bayer permission to amend their grounds of appeal.
Ground 1(1)
- Ground 1(1) is that the judge erred in law or principle by failing to apply the correct standard as to whether, on the basis of the cited prior art together with the common general knowledge at the priority date, it would have been obvious to the skilled team to include a once daily dosing arm in a rivaroxaban Phase II study with a reasonable expectation of success, namely a reasonable expectation that such a dosing arm would be both efficacious and safe for the treatment of a thromboembolic disorder.
- There are two stages to Bayer's argument in support of this ground. The first stage focusses on the judge's statements in [124] that there was no perceived technical barrier to the claimed invention on the part of the skilled team and that they would know that once daily administration of a wide range of doses would be likely to find the therapeutic window somewhere. Bayer submit that these statements are inconsistent with the judge's finding at [18], [120] and [125] that the skilled team would not know where the therapeutic window was or how wide it was, and with his finding at [176] that the skilled team would know that administering a relatively low dose at a relatively high frequency would give a better chance of staying safely inside the therapeutic window wherever that turned out to be. Bayer also submit that, in taking this approach, the judge was effectively asking himself whether there were reasons for the skilled team not to do what he had already assumed to be technically obvious in principle without even considering the prior art.
- I do not accept these submissions, which in my view are based on a misreading of what the judge was saying in [124]. All he was saying was that the skilled team would know that, in theory, a Phase II trial could be carried out with a wide range of once daily doses from small to large. If one adopted such a "scattergun" approach, there would be a good chance that one or more doses would turn out to lie within the therapeutic window. But as he immediately went on to say in [125], the skilled team would know that the problem with adopting such an approach was precisely that the location and size of the therapeutic window were unknown, and thus there was a real risk that some of the doses would fall outside it and hence patients would be harmed. Therefore the skilled team would not adopt such an approach.
- Although the judge did not spell the point out, it should be remembered that the claim is not limited to a particular size of dose. If it would be obvious to try any size of dose once daily with a reasonable prospect of success, then the claim is invalid. As can be seen from the judge's analysis at [249]-[258], however, the ultimate question in this case is whether, having read Harder and the Kubitza posters, the skilled team would have a reasonable expectation that once daily administration of a 30 mg dose would be efficacious and safe.
- The second stage of Bayer's argument focusses on the judge's statements in [129], [240] and [242] that the real or key criterion was whether the skilled team would have thought that it was worth applying to the relevant ethics committee for permission to conduct a Phase II trial which included a once daily regimen with a reasonable expectation that the committee would give permission and whether it was likely that the committee would have given permission. As the judge acknowledged at [130], neither side had argued this.
- It is not in dispute that approval from an ethics committee would have been required in order to carry out a Phase II trial of rivaroxaban or that the skilled team would have been aware of that. Nor is it in dispute that Bayer did obtain such approval to carry out the trial reported in the Patent (which, it may be noted, involved a 12-fold range of dose sizes). Bayer's argument is that this is legally irrelevant because the issue on inventive step is a purely technical one: would the skilled team have a reasonable expectation that a once daily regimen would be successful in terms of efficacy and safety?
- Given that, on Bayer's own case, consideration of the prospects of success in this context includes consideration of the safety of the patients who are to be enrolled in the Phase II trial, I can understand why the judge referred to the need for ethics committee approval. I agree with Bayer that on a strict legal analysis this is irrelevant, but as the judge pointed out at [130] the two-part criterion he discussed at [129] could be regarded as amounting to the same thing as the criterion identified by the parties in argument. This is because, on the facts of this case, success in terms of efficacy and safety would mean that the patients were not exposed in the Phase II trial to an unacceptable risk of being either under-dosed (potentially leading to thrombi) or over-dosed (potentially leading to excessive bleeding).
- Even if the judge would have been better advised not to refer to the need for ethics committee approval, this does not undermine his evaluation of obviousness. The judge repeatedly identified the correct legal criterion at [118], [130] and [241]. Most importantly, the question he asked himself at [245] and answered in the succeeding paragraphs was the correct question.
Ground 5
- As formulated in argument, ground 5 is that the judge failed to grapple with the key question of whether the skilled team would have a reasonable expectation, based on Harder and the Kubitza posters, that a once daily 30 mg dose of rivaroxaban would have a therapeutically useful effect for 24 hours. Bayer contend that, if the judge had grappled with this question, he should have answered it in the negative.
- Bayer's submissions in support of this ground amount to no more than a series of disagreements with the judge's reasoning at [249]-[257] without identifying any error of principle. For example, Bayer argue that the judge should have concluded that the half-life data in the Kubitza posters pointed against once daily dosing and that the PD data in Harder and the Kubitza posters did not demonstrate anticoagulant activity for 24 hours. The judge gave careful consideration to these arguments, however, and explained why, based on the evidence, he took a different view. Furthermore, contrary to Bayer's contention, the judge did squarely confront the question he is claimed not to have addressed. His answer at [256], based on his prior findings at [249], [251], [252] and [253], was that the data in Harder and the Kubitza posters gave reasonable grounds for the belief that once a daily dose of 30 mg would be likely to have a sustained antithrombotic effect over 24 hours and would not be likely to cause excessive bleeding.
- It is also worth noting that, as counsel for the Respondents pointed out, even Prof Meibohm's fall-back position was that twice daily doses of 20 mg and 30 mg would be tried. The 30 mg twice daily dose would have the same peak-to-trough variation as 30 mg once daily, but at a higher steady state concentration. Compared to a regimen of 30 mg twice daily, a regimen of 30 mg once daily would be expected, absent knowledge of where the therapeutic window lay, to lead to a lower risk of bleeding, but a higher risk of thrombi. Thus the key issue was whether 30 mg once daily would have a sufficient thrombotic effect. The evidence of Prof Hirsh and Prof Wilkins, which the judge accepted, was that the PD data in Harder and the Kubitza posters suggested that it would do. They formed that opinion before reading the Patent, and thus (so far as possible) without hindsight.
The unpleaded ground
- Bayer's unpleaded ground of appeal is that the judge's acceptance of the evidence of Prof Hirsh and Prof Wilkins in preference to that of Prof Crowther and Prof Meibohm was inconsistent with his rejection of Prof Hirsh's evidence that the skilled team would have made predictions as to the therapeutic window of rivaroxaban based on LMWHs and other FXa inhibitors because the judge was not satisfied that the materials relied upon by Prof Hirsh were common general knowledge. I do not accept this argument. It does not affect Prof Wilkins' evidence. Moreover, even in the case of Prof Hirsh, it does not affect the main thrust of his evidence as to what the clinician would take from Harder and the Kubitza posters. It is commonplace in patent cases for judges to accept the main thrust of expert witnesses' evidence without accepting their evidence on every point. Finally, this is nothing to do with the principal reason why the judge preferred the evidence of Prof Hirsh and Prof Wilkins to that of Prof Crowther and Prof Meibohm. As I have noted above, this was because even counsel for Bayer had felt unable to support the primary position taken by Prof Crowther and Prof Meibohm. I would therefore refuse Bayer permission to raise this ground.
Grounds 1(2) and (3)
- Grounds 1(2) and (3) were refined to a single point in argument, namely that the judge erred in placing weight on Bayer's decision not to adduce "invention story" evidence in this jurisdiction. Obviousness is to be objectively assessed from the perspective of the skilled person or team. The manner in which the inventor(s) actually arrived at the invention is legally irrelevant, and it is very rare for evidence from the inventor(s) to be adduced.
- The short answer to this argument is that the judge did not place any weight on the absence of "invention story" evidence in reaching his conclusion as to obviousness. As the judge explained, the principal relevance of the "invention story" advanced by Bayer in other jurisdictions, but not in this one, was that it provided an additional reason to the basic reason identified by the judge at [139] for not finding the decisions of foreign courts and tribunals in favour of Bayer persuasive. (Bayer did not rely upon any of those decisions in support of the appeal.) It is true that the judge returned to the point at [260], but that was after he had already made his finding of obviousness and when addressing the submission that Bayer must have had more data than is reported in Harder and the Kubitza posters (a submission that on Bayer's own argument was legally irrelevant as well as evidentially unsupported).
Conclusion
- The judge made no error of principle in his assessment of obviousness. His conclusion was grounded in the expert evidence. Nor, standing back, is that conclusion at all surprising. Harder expressly suggests that rivaroxaban is suitable for once daily administration. Harder and the Kubitza posters contain some data to support that statement, at least in the case of a 30 mg dose. It was therefore obvious to try including a once daily regimen in the Phase II trial, and the skilled team would have had a reasonable expectation that a 30 mg once daily dose would be efficacious and safe.
Postscript
- In October 2021 the Technical Board of Appeal of the European Patent Office upheld the validity of the Patent over a number of oppositions. From that date the Respondents knew that they had two and a half years in which to obtain an order for revocation of the Patent if they wished to clear the way for marketing rivaroxaban for once daily administration after 1 April 2024. The first claim form seeking revocation of the Patent was filed by three of the Respondents a full year later in October 2022. Other claim forms followed later still. The claims were joined and progressed without any expedition. In consequence, the trial was fixed for hearing dates that ended about five and a half weeks before 1 April 2024. On the first day of trial, counsel for the Respondents informed the judge that the claims had been case managed so as to try to ensure that judgment could be handed down before 1 April 2024. The judge was not informed, however, of the potential consequences if he was unable to meet that target. Nor did the Respondents give any apparent consideration to the potential for an appeal by Bayer.
- In the event, it became clear by late March 2024 that the judge would be unable to give judgment by 1 April 2024. This led to a heavily contested application by Bayer for a short-term interim injunction to restrain a number of the Respondents from marketing rivaroxaban for once daily administration until judgment was given. The judge acceded to that application for the reasons he gave in a judgment dated 27 March 2024 [2024] EWHC 711 (Pat). When the judge gave judgment on 12 April 2024, he was then predictably faced first with a contested application by Bayer for permission to appeal (which he refused) and then with a contested application by Bayer for a continuation of the interim injunction for a short period (which he granted) to enable Bayer to make applications to this Court for (i) permission to appeal, (ii) expedition of the appeal and (iii) continuation of the interim injunction until determination of the appeal. Bayer duly made those applications. The Respondents contested applications (i) and (iii), and both sides filed further evidence in support of and in opposition to application (iii). After considering these applications on paper, I granted all three.
- This flurry of applications for interim injunctive relief was not a sensible use of the resources either of the parties or of the courts. This situation could and should have been avoided by the Respondents bringing proceedings earlier than they did, or at least keeping the Patents Court properly and timeously informed as to the significance of the date of 1 April 2024.
Lady Justice Falk:
- I agree.
Lady Justice Nicola Davies
- I also agree.
