Covid-19 Protocol: This judgment was handed down remotely by circulation to the parties' representatives by email and release to BAILII. The date and time for hand-down is deemed to be Tuesday 8th June 2021 at 10am.
HHJ Nigel Lickley QC sitting as a Deputy Judge of the High Court:
- This is an application made by the Defendant pursuant to CPR 17.1(2) and PD 14 Paragraph 7 to resile from an admission of breach of duty, made in the Defence in this claim, to amend the Defence (to plead a denial inter alia to the allegations of breach of duty with respect to a 2 week wait referral); and to extend time for service of medical evidence. The second and third parts of the application stand or fall with the first. The application to resile is opposed.
- The application was made on the 18th December 2020 and was first listed and adjourned on the 10th May 2021. I heard the matter on the 19th and 26th May 2021 allowing the parties to submit evidence in the time between those two hearings. The reason for the listing delay from December 2020 to May 2021 I understand, arises from listing difficulties and the working of the QBD during the pandemic and the second national lockdown starting in late 2020. That additional delay is no fault of the parties however it is a factor to be considered as the trial of this matter is listed in October 2021.
The Background
- The Claimant's claim arises out of consultations he underwent with the Defendant on four occasions, namely 20th July 2015, 17th August 2015, 8th September 2015 and 29th September 2015. The Defendant was a Registered Nurse Practitioner working at the Lister Medical Centre, Lister House Health Centre Harlow. Given the nature of this application the first appointment is at the centre of the dispute.
- The Claimant, who was born on the 9th July 1951, attended the Health Centre on the 20th July 2015 complaining of a sore throat, a dry mouth and a neck lump that had, he says, been present, since before his birthday. There is a factual dispute as the note made referred to the lump being present for three days. The Defendant noted a '4cm Cyst like lump under the rt mandibular'. The full note of the examination is:
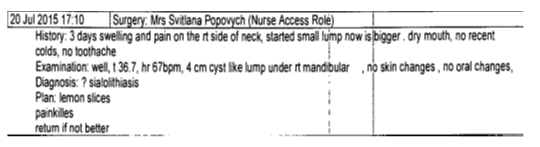
- The Claimant was told he had a suspected blocked saliva duct (Sialolithiasis) and was advised to suck lemons (a recognised treatment for the diagnosed condition). No tests, investigations or referrals were arranged.
- The NICE guidelines introduced on 23rd June 2015 provided that in such circumstances:
"Head and neck cancers
Laryngeal cancer
1.8.1 Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for laryngeal cancer in people aged 45 and over with:
persistent unexplained hoarseness or
an unexplained lump in the neck.
Oral cancer
1.8.2 Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for oral cancer in people with either:
unexplained ulceration in the oral cavity lasting for more than 3 weeks or
a persistent and unexplained lump in the neck."
- Throughout the period in question (July to September 2015) when the Defendant saw the Claimant the neck lump grew in size. The lump later transpired to be a squamous cell carcinoma requiring surgery. The Claimant has been left with disabilities as a consequence of that surgery. It is accepted that surgery would have been necessary in any event, however the claim concerns the delay in that surgery caused by the negligent assessments and late referral to a specialist team made by the Defendant. In short surgery was delayed by negligence and as a consequence the lump was larger requiring more invasive surgery than would otherwise have been the case had the Defendant acted with proper and appropriate skill and care.
- There is no dispute that the Defendant did not consider or apply the NICE guidance that given the findings on the 20th July 2015 the Claimant required a referral. It is not suggested the Defendant was even aware of the NICE guidance. Ultimately the Claimant was first referred to a specialist on the 14th September 2015. As a consequence the Claimant was seen first by Mr Coglan on the 15th October 2015. Following further assessments the Claimant underwent surgery on the 12th November 2015 involving biopsy of the base of the tongue, extraction of three teeth and a right modified radial neck dissection. During surgery he suffered damage to the spinal accessory nerve, the sympathetic chain and the marginal mandibular branch of the facial nerve on the right side. As a consequence the Claimant suffers from loss of function to the right shoulder and arm. He also suffered damage resulting in Horner's Syndrome causing his right eyelid to droop and loss of sensation to the right ear. Subsequently the Claimant underwent post-operative radiotherapy and Chemotherapy. Mr Reece FRCS an ENT Consultant relied upon by the Defendant in his report of 15th January 2021 stated at Paragraph 4.03 "if the Claimant had been referred on the 20th July 2015 and thereafter progression to surgery at the same rate that actually occurred the Claimant would have been operated on 3rd September 2015".
Procedural history
- A chronology has been prepared setting out the procedural history. In summary - A Letter of Claim was served on the 3rd July 2018. There was no response from the Defendant. Accordingly the Defendant failed to comply with the pre-action protocol. The Claim Form was issued on the 30th August 2019.
- The Particulars of Claim dated 19th December 2019 (deemed served on 23rd December 2019) alleged particulars of negligence relating to the occasions when the Claimant saw the Defendant during 2015 and generally. I will turn to the specific allegations later in this judgment when considering the liability report of Nurse Wiltshire (dated February 2020) relied upon by the Defendant but not served as part of the case given that Nurse Wiltshire concluded that the Defendant was negligent on the 20th July 2015 in a number of respects including failing to refer the Claimant in accordance with the NICE guidelines and on occasions thereafter. It is a change in her opinion about the conduct of the Defendant only on the 20th July 2015 that is central to this application. In relation to the other occasions there is no change in her assessment and position the Defendant was negligent and in breach of duty.
- Liability was admitted in the defence dated 26th March 2020 (served on 1st April 2020) in relation to the first appointment on the 20th July 2015 in that the Defendant failed to refer the Claimant in accordance with the NICE guidelines for patients presenting with neck lumps for investigation and treatment given the potential for the lump to be cancerous namely that she failed to make a 2-week wait referral on the suspected cancer pathway (Para 18). In light of that admission no additional admissions or responses were made to the other general allegations and those regarding the other appointments given the concession made. For reasons I will come to, the Defendant was undoubtedly negligent on other occasions. It is not contended otherwise on her behalf. Given the admission the case proceeded upon that basis. I add that no witness statement has been served or relied upon from the Defendant herself although one exists as appears from the Nursing expert report.
The Application and the evidence relied upon
- The Defendant seeks to resile from the admission of liability made in March 2020. In order to do so an explanation has been provided as to why the admission was made in the first place. Ms Owen, who has conduct of the matter on behalf of the Defendant, in her witness statement dated 18th December 2020 has sought to explain what occurred.
- She stated:
"Prior to drafting of the Defence, the Defendant obtained expert evidence from a nursing expert, Nurse Wiltshire. A copy of her report is attached as Exhibit AO2. It can be seen from that document that Nurse Wiltshire advised that the Defendant was in breach of duty for failing to refer the Claimant urgently on 20th July 2015 in accordance with the NICE Guidelines. It can also be seen that Nurse Wiltshire makes no reference to any local guidance surrounding referral of neck lumps."
And
"Given the consequences of an admission in the Defence, great care was taken by me, before the Defence was finalised to ensure the admission being made was correct. I attach as Exhibit AO3 a copy of an email I sent to Nurse Wiltshire to fully clarify the position with respect to this admission before it was made and her response confirming there was a breach of duty for failing to follow the NICE guidance on this date. In light of the information received from Nurse Wiltshire, an admission with respect to a failure to refer under the two week wait pathway was made in the Defence at paragraph 18. No other admissions were made as to breach of duty and the Claimant did not seek to press for admissions or otherwise with respect to the other allegations"
Nurse Wiltshire's report of February 2020
- At paragraph 4.1 under the heading 'Good Practice' the expert stated that "All NP's ...nurse practitioners) should be aware of and follow current NICE and local guidelines". It is said therefore that the Defendant was on notice as to the issue of local guidance from this point at least. It appears the Defendant was unaware of any local guidelines and therefore had not mentioned them and so they were not sought. The expert then set out what a clinician should do in circumstances where a patient presents with an unexplained lump in the neck. Having considered the evidence the expert set out her conclusions and did so by following the particulars of negligence. The expert concluded given the presentation and symptoms of the Claimant:
(i) That there was sub-standard care in failing to adequately consider an explanation other than a blocked salivary gland (those other explanations include cancer).
(ii) That the Defendant, by failing to be aware of the NICE guidelines and act in accordance with them, provided sub-standard care.
(iii) Given that the Claimant met the criteria for referral under the 2-week wait, failure to refer fell below the standard of care expected of a competent NP.
(iv) That there was a failure to note the site of the lump, if it was fixed or mobile and whether there were abnormalities on the neck.
(v) That there was a failure to assess the neck lump to determine if it was fixed, hard or tender and to document the findings and this represented sub-standard care.
(vi) The Defendant was incorrect to diagnose Sialolithiasis given the symptoms and history.
(vii) The Claimant should have been referred to specialist care sooner than he was.
Other criticisms concern other sub-standard care and failures to refer on other occasions.
- At a CCMC on 23rd July 2020 before Master Yoxall permission was given to the Defendant to obtain causation evidence from Mr Reece, consultant ENT surgeon. Mr Reece was not instructed to provide evidence with respect to breach of duty. Ms Owen states that of his own volition Mr Reece volunteered on 26th July 2020, that he was aware of a local protocol for referral of suspicious neck lumps which suggested that such lumps should be referred on or after they had been present for 3 weeks. In other words the local guidance was at odds with the NICE guidance and the local guidance would be followed thus meaning the failure to refer was not, of itself, a breach of duty.
- A copy of the local guidance was sent to Ms Owen after further delay on the 10th September 2020. A copy of two documents has been provided first, a Suspected Head and Neck cancer referral form is a check list / template for hospitals in north and central London dated 17th June 2015 that refers in the section headed 'Clinical Details" to 'Lump in neck Unresolved neck masses for more than three weeks' and second, a flow chart dated 2014 for 'Head and Neck cancer referral guidelines' that advises an urgent referral to the head and neck team in cases of 'unexplained lump in neck recently appeared or changed over 3-6 weeks'. In addition a referral is necessary in cases of 'unexplained persistent sore throat' and 'unexplained persistent swelling in the parotid or submandibular gland'.
- Nurse Wiltshire was also asked about the local guidance by email on the 9th September 2020. In her reply of 17th September 2020 the expert said that she was not aware of any local guidance and had based her opinion on the NICE guidelines of June 2015 and according to the Claimant the lump had been present for 11 days and so a referral was indicated. She added "if the local guidelines state that an unexplained neck lump should be present for 3 weeks before referral and the practice followed these guidelines then the referral was not indicated on 20 July 2015'.
- The guidelines as we have them were sent to the Nursing expert on the 7th October 2020. Her reply sent on the 8th October 2020 stated 'based on the local guidelines Nurse P was not in breach of her duty of care on 20 July 2015 as the lump in the Claimant's neck had not been present for more than three weeks.' Nurse Wiltshire added that there was a breach of the duty of care to refer on the 17th August 2015.
- Witness evidence was served by the Claimant commenting only on the issues of condition, prognosis and quantum on the 1st October 2020. The parties were due to serve expert evidence on causation on the 23rd October 2020.
- The newly obtained guidance was sent to the Claimant's solicitors on the 16th October 2020. Ms Owen by letter asked for time to consider the effect on the case of the apparent change in position and asked for an extension of 28 days to serve the causation evidence and consider the guidelines with their expert. A new date was agreed to simultaneously exchange expert evidence on the 20th November 2020. On that date, Miss Winch, the solicitor for the Claimant, in her witness statement of the 19th March 2021, states that the Defendant requested a further two month extension of time to the 20th January 2021. An agreement was reached to serve the evidence on the 18th December 2020. According to the chronology prepared by Miss Heyworth from the 16th October 2020 when the guidance was sent to the Claimant, nothing happened for two months until a conference was held with counsel on the 11th December 2020.
- The application to amend was made on the 18th December 2020. On the 18th December 2020 the Claimant served their causation, condition, prognosis and quantum evidence. The causation reports were password protected until such time as the Defendant served their reports. Eventually the Defendant served their causation evidence on the 29th January 2021.
- Mr Reece in his expert report of 15th January 2021 has stated:
(i) Paragraph 3.01: He agreed with the Particulars of Claim that the Claimant's history and symptoms were not consistent with Sialolithiasis.
(ii) Paragraph 3.03: Having referred to the NICE guidelines he said that the local guidelines at the time suggest that an unexplained neck lump present for three weeks should be referred on the suspected Head and Neck Cancer Pathway. I note his use of the word 'suggest'.
(iii) Paragraph 3.05: That UK guidelines at the time for cancer treatment were that a patient should be seen by a specialist within two weeks of a referral by a GP with suspected cancer.
(iv) Paragraph 4.01 and 02: He concluded given the local guidance that it was reasonable not to make a referral on the 20th July 2015 as the conflict concerning the duration of the lump (11 or 3 days) 'makes no difference'. He added in his opinion 'it is not reasonable that the Defendant did not make the referral on the 17th August 2015 because the lump had been present for over three weeks' and if referred then 'the Claimant would have been operated on 15th October 2015'.
(v) Paragraph 6.02: The Claimant presented (according to the note) with a three day swelling and pain in the neck. Local guidelines did not require the Claimant to make an urgent suspected head and neck referral at that time. Given that the signs and symptoms persisted on the 17th August 2015 an urgent referral was warranted.
(vi) Paragraph 4.03: He said that if the referral had taken place on the 20th July 2015 surgery would have been on the 3rd September 2015. A neck dissection would still have been undertaken however it would not have been so complicated and damage to the accessory nerve, the marginal mandibular nerve and sympathetic chain would probably not have occurred. There would still have been the need for radiotherapy and chemotherapy with resultant difficulties in swallowing.
(vii) Paragraph 4.04: A referral on the 17th August 2015 would have meant a less extensive neck dissection than was eventually necessary but would have meant sacrifice of the accessory nerve and sternocleidomastoid muscle. The Claimant would not however have suffered from Horner's syndrome.
- No other medical expert has commented on this issue given that liability was conceded.
- I allowed the parties time to adduce additional evidence between the two hearings before me given the issues raised. Finally, I was provided with a letter from Nurse Wiltshire dated 25th May 2021. In that letter she confirmed that she had read the guidelines and, in accordance with that guidance, a referral was not indicated on the 20th July 2015. She added that the guidance referred to a referral in the case of persistent sore throat or swelling in the submandibular gland however as there was no note of such in the medical records no referral was indicated on that basis either.
- What is not apparent is if the new conclusion affects her overall position as set out in her report as to other areas of 'sub-standard' care. Namely the wrong diagnosis, failure to examine and record properly and consider other potential causes that include cancer (section 4.1 Causes of neck lumps). I take it and will proceed on the basis that there being no comment from Nurse Wiltshire that there is no change in her opinion on those topics namely that the Defendant did provide sub-standard care i.e. was negligent in these regards on the 20th July 2015 as she concluded.
- Apart from the further evidence from Nurse Wiltshire no evidence has been adduced before me to suggest that the Health Centre adopted the purported local guidance as Nurse Wiltshire suggested or that the Defendant was aware of the local guidance and acted in accordance with it. No other material has been provided. The first document of local guidance has a link to the guidance but that has not been provided. One assumes there is overall guidance how to use and interpret etc. Quite why the documents have different dates has not been explained. I therefore proceed on the basis that the guidance had not been adopted by the surgery and that the Defendant was unaware of both the NICE guidelines and any local guidance and accordingly did not purport to act in reliance on any such guidance.
The application
- The Defendant seeks to resile from the admission made. An amended defence has been provided. The Defendant seeks to withdraw from the admissions made both as to breach of duty and causation in the Defence. Permission is required to do so as the defence has been served.
- CPR 17 sets out the test required for amendments to Statements of case:
"Amendments to statements of case
17.1
(1) A party may amend his statement of case at any time before it has been served on any other party.
(2) If his statement of case has been served, a party may amend it only
(a) with the written consent of all the other parties; or
(b) with the permission of the court.
(3) If a statement of case has been served, an application to amend it by removing, adding or substituting a party must be made in accordance with rule 19.4.
(Part 22 requires amendments to a statement of case to be verified by a statement of truth unless the court orders otherwise)"
- The Practice Direction to CPR14 sets out the test that needs to be considered upon an application to withdraw an admission:
"Withdrawing an admission
7.1 An admission made under Part 14 may be withdrawn with the court's permission.
7.2 In deciding whether to give permission for an admission to be withdrawn, the court will have regard to all the circumstances of the case, including
(a) the grounds upon which the applicant seeks to withdraw the admission including whether or not new evidence has come to light which was not available at the time the admission was made;
(b) the conduct of the parties, including any conduct which led the party making the admission to do so;
(c) the prejudice that may be caused to any person if the admission is withdrawn;
(d) the prejudice that may be caused to any person if the application is refused;
(e) the stage in the proceedings at which the application to withdraw is made, in particular in relation to the date or period fixed for trial;
(f) the prospects of success (if the admission is withdrawn) of the claim or part of the claim in relation to which the admission was made; and
(g) the interests of the administration of justice."
- I deal with each of the above in turn and summarise the submissions made:
(a) the grounds upon which the applicant seeks to withdraw the admission including whether or not new evidence has come to light which was not available at the time the admission was made;
The Defendant says the new evidence in the form of the local guidance came to light when Mr Reece referred to it. Prior to that it was not available. At no point was it brought to the attention of the solicitors by Nurse Wiltshire or the Defendant. Now that it is available it is important and shows that a body of Nurse practitioners would not have referred the Claimant on the 20th July 2015 as the guidance required a neck lump to be present for three weeks before referral. Accordingly it is argued that even though the Defendant was unaware of the guidance it matters not because a referral would not be required in short the result is the same because a reasonably competent Nurse in the Defendant's position and given the circumstances would not have referred the Claimant to a specialist. It is said this is genuinely new evidence.
The Claimant says the evidence was there to be found if the Defendant had looked for it. The conclusion they suggest is that because the Defendant made no mention of local guidance because it played no part in her reasoning it was not sought. In addition, Nurse Wiltshire did refer to local guidance in her report as something to be followed and adopted by the Defendant. It amounts to an admission made after inadequate investigation it is said.
(b) the conduct of the parties, including any conduct which led the party making the admission to do so;
The Defendant says that once the new material was brought to their attention matters progressed quickly. In fact it took from July to December 2020 for an application to be made. It is said the Claimant waited until near to the end of the limitation period to issue his letter of claim and then waited for nearly a year to issue proceedings. Finally, the Defendant says the issue was progressed promptly once clarified.
The Claimant says the Defendant did not comply with the pre-action protocol, no material was supplied to the Claimant from July 2018 to enable the claim to be investigated, the admission was made in the defence of March 2020 and it is said the conduct of the Defendant is delaying resolution of the matter. There is no suggestion the Claimant has acted in any way to have caused the admission to be made.
(c) the prejudice that may be caused to any person if the admission is withdrawn;
The Defendant says there were ten months to trial when the application was made and that there is little or no prejudice to the Claimant if the admission is withdrawn. Although the Claimant will have to provide a witness statement (as will his wife) as to the facts and go back to July 2015 to do so, a witness statement as to the facts must have been taken before proceedings were commenced and that can be used now. It is said the Claimant can give evidence about the consultation on the 20th July 2015 and what he said about the duration of the neck lump. Further the Claimant would have obtained expert evidence on breach of duty prior to issue of the claim given the principles expressed in Pantelli Associates Limited v Corporate City Developments [2010] EWHC 3189 (TCC)and therefore an expert is available to give the necessary evidence. Therefore the issues can be resolved in court. The trial need not be vacated it is said and a strict timetable will permit the case to go ahead in October 2021.
The Claimant says to withdraw the admission on the key issue of liability now will cause prejudice. It will cause stress and uncertainty in terms of recovery of compensation, the trial will have to be vacated and the Claimant will have to revisit the events of nearly six years ago in the context of his treatment for cancer.
(d) the prejudice that may be caused to any person if the application is refused;
It is said that if the Defendant is not allowed to amend and withdraw the admission she is deprived of a good breach of duty Defence for the consultation of 20th July 2015. The evidence now supports an argument that a reasonable body of Nurse Practitioners would not have referred on that day and that makes a considerable difference to the claim. It is said that given that the issues relate to delay in identification and treatment of cancer it is plain that the earlier consultation dates are the key dates to consider with respect to the causation position. It is said to be central to the case that the consultation date of 20th July 2015 is the only date by which the Claimant has any argument that referral and treatment may have occurred before mid-September. If in fact the failure to refer then was not negligent treatment surgery would have been delayed as a consequence with the Claimant still suffering unavoidable surgical damage as a result. It is said the determination of this important issue may affect the quantum of damages awarded and the Defendant should not be deprived of a legitimate argument. Finally, it is said the claim has grown from £59,000 at the time the admission was made to now nearly £627,000 and the Defendant should be able to meet the enlarged claim by allowing the application.
The Claimant says in essence this issue is bound up with the prospects of success if the admission is withdrawn and the issue is litigated. The Claimant says even if the issue is litigated the Claimant will succeed because of the Defendant's negligence in August 2015 and the defence will ultimately fail. It is said all that will happen is that the Claimant will suffer further delay to the recovery of damages.
(e) the stage in the proceedings at which the application to withdraw is made, in particular in relation to the date or period fixed for trial;
The trial of this matter is to commence on the 4th October 2021. That is just short of two years after the Particulars of Claim were deemed served on 23rd December 2019 with the Defence filed on 1st April 2020. Directions were provided at CCMC on 23rd July 2020. It is said by the Defendant that disclosure has taken place and would not have altered, breach of duty evidence and joint statements along with updated witness evidence can be provided without disrupting the Court time table.
The Claimant says the case will change and be a fully disputed breach, causation and quantum case from what was expected to be essentially a quantum only case. In effect a totally different case to the one anticipated. In order to respond to any amended defence further investigation will be necessary, a new particulars of claim will be needed, additional witness statements and expert opinion. All of that would have to be timetabled meaning the trial will have to be vacated. A trial might be longer with more witnesses and experts.
(f) the prospects of success (if the admission is withdrawn) of the claim or part of the claim in relation to which the admission was made;
The Defendant says the evidence as it now stands remains uncontradicted by the Claimant and establishes an arguable case that a reasonable body of Nurse Practitioners would not have referred the Claimant on 20th July 2020. It is submitted the prospects of success on the point, and on causation flowing from it are good. For completeness whilst other admissions have been made in the amended Defence, no causation flows from these and as such the prospects of success regarding the claim as a whole remain good.
Miss Heyworth argues that it is irrelevant that the Defendant did not know of the local guidance (or the NICE guidance) and does not seek to justify her decisions by relying upon it. She also submits that it matters not that the Health Centre did not adopt the guidance. Her essential point is that when looking at a reasonably competent person in the Defendant's position according to two experts no referral was required on the 20th July 2015. Therefore it is said there is no breach of duty whatever the motivation or decision making processes of the Defendant at the time. Miss Heyworth submits that when looking at the timelines for assessment and surgery on the available evidence, at best, the Claimant fails to meet the deadline for surgery in early August.
Mr Williamson for the Claimant says it is important that the Defendant did not follow the guidance as Nurse Wiltshire has stated that guidance should be followed. In addition Nurse Wiltshire stated that any breach is conditional upon the Health Centre following the guidelines. Accordingly it is said there is no evidence the guidelines were in place at the Health Centre or in fact anywhere else in the UK at the time. Further it is said the two forms are contradictory given that the flow chart refers to an 'unexplained neck lump recently appeared or changed over 3-6 weeks' it being suggested the lump in question had recently appeared. If that reading is correct that is, it is said, consistent with the NICE guidelines.
Mr Williamson says the evidence of Nurse Wiltshire is also flawed in that in her recent statement where she says that there were no other symptoms meriting a referral in fact other symptoms were reported as being present being the submandibular swelling and the conclusion that the salivary gland was blocked when the Parotid gland is a salivary gland. In addition he submits that no assessment has been made of the other failures of care noted by Nurse Wiltshire in summary being a failure to examine, a negligent diagnosis of Sialolithiasis and a failure to consider cancer as a cause of the lump. In short he says no answer has been given to the following questions - but for the negligence in failing to accurately assess the Claimant's condition what would the Defendant have determined or advised? But for the negligence in failing to consider cancer as a possible cause what would the Defendant have attributed the presentation to? And but for the negligent diagnosis of Sialolithiasis what would the Defendant have considered? In essence he says there is more to it than a failure to refer. He says a reasonably competent nurse in the Defendant's position would not have made so many errors and would have followed a different route in terms of reasoning a route that takes you to cancer and different action. He says there is no reasonable prospect of success in the new argument advanced.
(g) the interests of the administration of justice.
The Defendant says the issue is live and needs to be resolved. The interests of justice favour the withdrawal of the admission and the amendment of the Defence in line with the attached draft.
The Claimant says the Defendant's conduct throughout undermines the administration of justice. The admission was made after careful consideration and clarification of the evidence and after taking expert advice. The admission was based upon the Defendant's own knowledge. It is said the overall conduct of the Defendant is contrary to good practice, was made after delay and is late. The trial date is in jeopardy with the court's resources allocated in October 2021 put at risk.
Decision
- I have considered the helpful submissions of counsel. Having considered all that has been said, applying the factors set out in the Practice Direction and exercising my discretion, I refuse to allow the Defendant to make the amendment sought. I do so for the following reasons:
(i) The local guidance as provided was available in a strict sense at the time the case commenced. It was not known about and not sought. It took the Defendant from July 2020, when the issue was first raised by Mr Reece, until December 2020 to make the application. Nurse Wiltshire did not conclude her comments until October 2020. The failure to comply with the pre-action protocol cannot be overlooked. Quite why the issue of local guidance was not considered at an earlier stage is difficult to understand. Experienced solicitors in this field would, I assume, have been aware of the existence of local guidance albeit in general and Nurse Wiltshire referred to such guidance in her report. Quite why she did not know of the guidance as an expert or put the Defendant on notice to investigate the issue is equally difficult to fathom. Accordingly there has been inadequate investigation and considerable delay in bringing the application from July to December 2020.
(ii) The greater prejudice in my judgement would fall upon the Claimant if I were to allow the application. On any assessment of the work needed to bring the issue to trial I am forced to conclude that the trial date will have to be vacated. That means more delay and uncertainty for the Claimant who hitherto had assumed his case would proceed on the basis that liability was not in dispute. He has been of that mind for over a year. The case he would have to now prepare for would be markedly different to the one he has anticipated. That will bring undoubted stress through no fault of his own. I appreciate that the Defendant will not be able to run the new causation argument, however the greater prejudice falls firmly against amendment.
(iii) Prospects of success. In my judgement the point raised lacks any real prospect of success. I come to this conclusion for the following reasons:
(a) The Defendant, according to Nurse Wiltshire, provided sub-standard care in a number of ways on the 20th July 2015 and thereafter. The Defendant was negligent in failing to refer in August 2015 in any event. The Defendant therefore cannot completely escape liability by the amendment sought. The amendment goes to limiting the claim.
(b) The evidence adduced, on my assessment, falls short of dealing with the overall picture, focusses only on the narrow referral issue and is accordingly unsatisfactory and lacking. The issue of breach of duty is more nuanced and complex than is suggested. While it is said the evidence shows that a body of nurses would not have referred in the Claimant's case because of the local guidance the evidence falls short of informing what a reasonably competent nurse would in fact have done given the Claimant's presentation. I cannot determine what a reasonably competent nurse in the Defendant's position would have done had she not been negligent in the other ways suggested other than to conclude that a cancer diagnosis would have been considered as it is suggested it should have been, Sialolithiasis would not have been diagnosed, the neck lump would have been examined and noted properly, the NICE guidance and any other local guidance would have been considered and a decision made. Nurse Wiltshire has not dealt with these important issues. These issues are not, as was said in submissions, 'cross-examination points'. They go to the validity of the opinion evidence relied upon and strength of the argument.
(c) There is no evidence the guidance was in force, adopted by the Health Centre and therefore applicable at the time. On the face of the documents supplied there is an apparent contradiction and the material is not complete. It is not suggested the Defendant was aware of the local guidance and acted in reliance upon it therefore how does Nurse Wiltshire square that with her point that competent Nurse Practitioners would follow such guidance?
(d) Finally, the recent letter from Nurse Wiltshire appears to have been written without proper consideration of the medical note made at the time and fails to consider accordingly if a referral was merited on other grounds in any event.
(e) Finally, even if I were wrong about the prospects of success, the delay and additional work necessary to litigate the issue is not justified and I would refuse the application for the other reasons stated.
(iv) Administration of Justice. The court service is under significant stress and pressure at the current time and resources have been set aside for this case to proceed to trial this year. There is also a wider public interest in the efficient discharge of court business with the avoidance of delays. Litigation should be conducted in a manner that incorporates that aim. The lateness of an important issue arising in this case, the time taken to make the application coupled with the other delays set out above will mean the trial will have to be vacated.
- For the reasons set out above the application is dismissed. I invite the parties to draw up the Order giving effect to this disposal and the effect on any extant applications before the court.